This is part of a series of posts reporting outcomes from a project on Agency in Youth Mental Health, led by Rose McCabe at City University. In the previous post, the project team explained why young people may have heightened risks of experiencing epistemic injustice in clinical encounters. Today, Clara Bergen and Rose McCabe provide evidence that young people's sense of agency is sometimes undermined in such encounters.

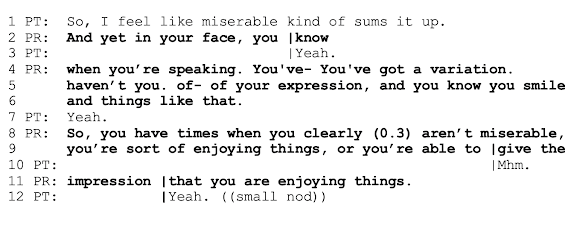
Rather than accepting Patrick’s [PT] description of his experience (feeling “miserable”, line 1), the practitioner [PR] cites Patrick's facial expressions (“you smile” lines 4-6) as evidence (“So” line 8) that he has “times when” he isn’t miserable (line 8) and is “enjoying things” (line 9). In this way, the practitioner cites contrasting information (lines 4-6) as evidence against Patrick’s description of himself as “miserable”.
The contrastive framing (“yet” line 2), lack of acceptance (e.g., okay), and assertion that Patrick isn’t always miserable (lines 8-9), discount Patrick’s characterization as untrue. Patrick responds minimally (lines 3, 7, 10), showing signs of disengagement (Peräkylä et al 2021) and passive participation without agreement. The practitioner concedes that the Patrick could just be giving the impression of enjoying things (lines 9, 11). At this point, Patrick nods, showing some affiliation with this last statement.
Practitioners feel a sense of powerlessness and burnout in the face of exclusionary referral criteria and long waiting lists (O’Keeffe et al 2021). This minimization of patient distress may be one consequence of forcing practitioners to ration overwhelmed mental health services.
National Health Service slogans like “just talking can help” and “don’t be afraid to ask for help” aim to encourage early intervention and help-seeking for mental health problems (Health and Social Care Committee 2021). However, the communication practices identified in this study undermine public health initiatives for early intervention, leaving patients to question whether they truly deserve care (Liberati et al 2022). Examples like Patrick's above help us understand why so many people seeking help for self-harm describe feeling excluded from services and “unworthy of help” (Xanthopoulou et al 2021).

By analysing video recordings of police interactions, courtroom cross-examinations, and political news interviews, researchers have learned a lot about how institutional figures challenge what other people have felt or experienced.
For example, police and lawyers use subtle practices like asking questions that imply inconsistency or implausibility (Stokoe et al 2020), anticipate a compromising response (Drew 1992), or imply disagreement (Jol & van der Houwen 2014). Lawyers and political interviewers may take an adversarial stance (Clayman & Heritage 2002) or imply that evidence suggests an alternative characterization (Antaki et al 2015).
In this study, we asked whether these communication practices are also used by practitioners in mental health services. We examined 46 video-recorded psychosocial assessments for people attending the Emergency Department with thoughts of suicide or self-harm.
In this study, we asked whether these communication practices are also used by practitioners in mental health services. We examined 46 video-recorded psychosocial assessments for people attending the Emergency Department with thoughts of suicide or self-harm.
 |
| Clara Bergen |
 |
| Rose McCabe |
What we found was striking – across these data, mental health practitioners used all these communication practices for challenging what a person had felt or experienced. Most often, practitioners used these practices to downplay a person’s distress or their risk of suicide. This aligned with what our young lived experience researchers described about their own interactions with mental health services.
This fits into a wider institutional context. In the Emergency Department, practitioners are under a lot of pressure to discharge patients quickly and there are limited inpatient beds and services in the community for people in distress. Practitioners are forced to take the role of gatekeeper (Fisher 2022) and ration referrals to overwhelmed mental health services.
See the example below. Patrick, an 18-year-old man, has come to the Emergency Department to get hel for suicidal thoughts. He describes himself as feeling miserable. We use Conversation Analysis, a way of micro-analysing verbal and nonverbal features of communication (see Sidnell & Stivers 2012), to analyse these data.
This fits into a wider institutional context. In the Emergency Department, practitioners are under a lot of pressure to discharge patients quickly and there are limited inpatient beds and services in the community for people in distress. Practitioners are forced to take the role of gatekeeper (Fisher 2022) and ration referrals to overwhelmed mental health services.
See the example below. Patrick, an 18-year-old man, has come to the Emergency Department to get hel for suicidal thoughts. He describes himself as feeling miserable. We use Conversation Analysis, a way of micro-analysing verbal and nonverbal features of communication (see Sidnell & Stivers 2012), to analyse these data.

Practitioners feel a sense of powerlessness and burnout in the face of exclusionary referral criteria and long waiting lists (O’Keeffe et al 2021). This minimization of patient distress may be one consequence of forcing practitioners to ration overwhelmed mental health services.
National Health Service slogans like “just talking can help” and “don’t be afraid to ask for help” aim to encourage early intervention and help-seeking for mental health problems (Health and Social Care Committee 2021). However, the communication practices identified in this study undermine public health initiatives for early intervention, leaving patients to question whether they truly deserve care (Liberati et al 2022). Examples like Patrick's above help us understand why so many people seeking help for self-harm describe feeling excluded from services and “unworthy of help” (Xanthopoulou et al 2021).